Chiropractic Clinical Outcomes Among Older Adult Male Veterans With Chronic Lower Back Pain: A Retrospective Review of Quality-Assurance Data
Chiropractic Clinical Outcomes Among Older Adult Male Veterans With Chronic Lower Back Pain: A Retrospective Review of Quality-Assurance Data
SOURCE: J Chiropractic Medicine 2022 (Jun); 21 (2): 77–82
| OPEN ACCESS |
Brian A. Davis, DC, Andrew S.Dunn, DC, MS, MEd, Derek J. Golley, DC, MS, Dave R. Chicoine, DC, MS
Chiropractic Department,
VA Western New York Healthcare System,
Buffalo, New York.
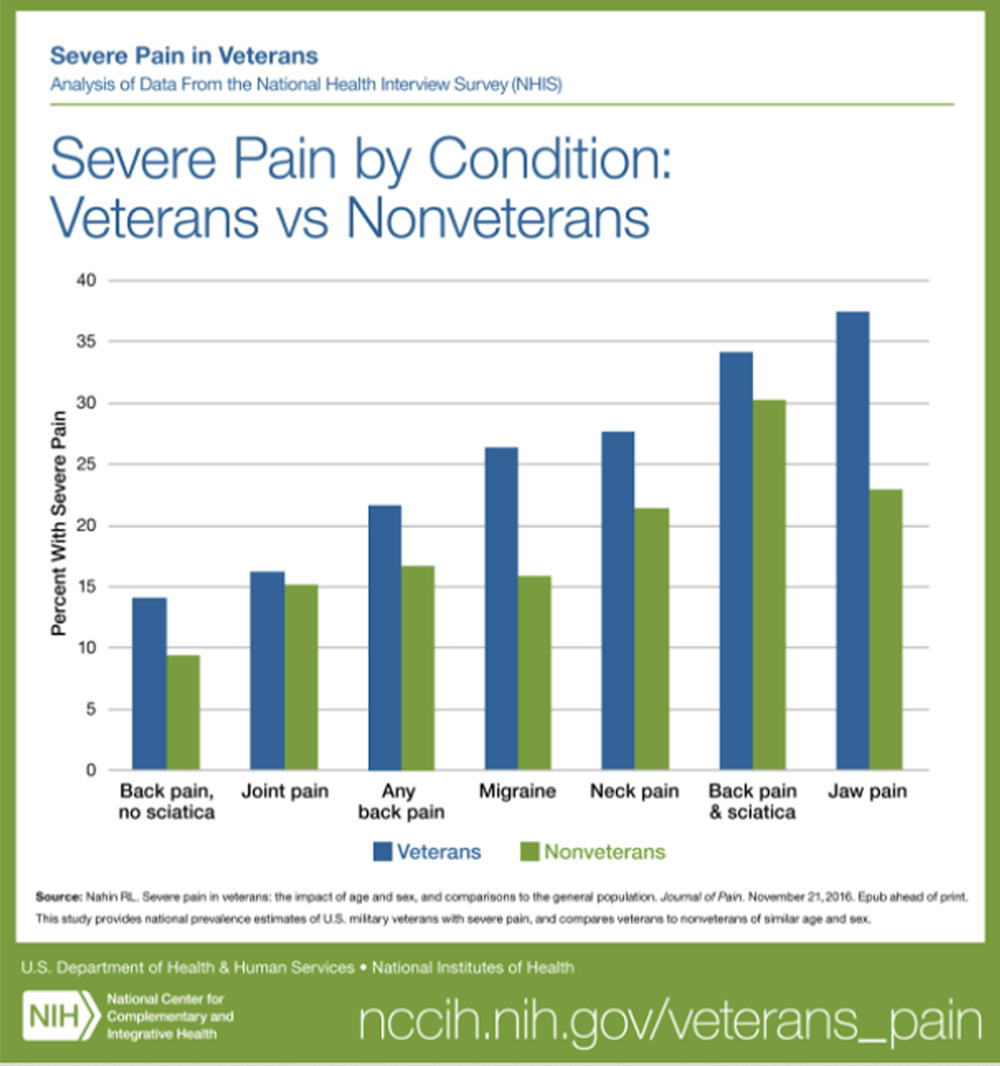
FROM: Nahin ~ Pain 2017
Objective: The purpose of this study was to determine whether a sample of older adult male U.S. veterans demonstrated clinically and statistically significant improvement in chronic lower back pain on validated outcome measures after a short course of chiropractic care.
Methods: We performed a retrospective review of a quality-assurance data set of outcome metrics for male veterans, aged 65 to 89 years, who had chronic low back pain, defined as pain in the lower back region present for at least 3 months before evaluation. We included those who received chiropractic management from January 1, 2010, to December 31, 2018. Paired t tests were used to compare outcomes after 4 treatments on both a numeric rating scale (NRS) and the Back Bournemouth Questionnaire (BBQ). The minimum clinically important difference (MCID) was set at 30% change from baseline.
There is more like this @ our:
NON-PHARMACOLOGIC THERAPY Section and the: