

Association Between Chiropractic Spinal Manipulation for Sciatica and Opioid-related Adverse Events: A Retrospective Cohort Study
SOURCE: PLoS One 2025 (Jan 28); 20 (1): e0317663
| OPEN ACCESS |
Robert J. Trager • Zachary A. Cupler • Roshini Srinivasan • Elleson G. Harper • Jaime A. Perez
Connor Whole Health,
University Hospitals Cleveland Medical Center,
Cleveland, Ohio, United States of America.
Background: Patients receiving chiropractic spinal manipulation (CSM) for spinal pain are less likely to be prescribed opioids, and some evidence suggests that these patients have a lower risk of any type of adverse drug event. We hypothesize that adults receiving CSM for sciatica will have a reduced risk of opioid-related adverse drug events (ORADEs) over a one-year follow-up compared to matched controls not receiving CSM.
Methods: We searched a United States (US) claims-based data resource (Diamond Network, TriNetX, Inc.) of more than 216 million patients, yielding data ranging from 2009 to 2024. We included patients aged ?18 years with sciatica, excluding those post-spine surgery, prior anesthesia, serious pathology, high risk of ORADEs, and an ORADE ? 1-year prior. Patients were divided into two cohorts: (1) CSM and (2) usual medical care. We used propensity score matching to control for confounding variables associated with ORADEs. Comparative outcomes were analyzed by calculating risk ratios (RRs) and 95% confidence intervals (CIs) for the incidence of ORADEs and oral opioid prescription between cohorts.
Results: 372,471 patients per cohort remained after matching. The incidence of ORADEs over 1-year follow-up was less in the CSM cohort compared to the usual medical care cohort (CSM: 0.09%; usual medical care: 0.30%), yielding an RR of 0.29 (95% CI: 0.25-0.32; P < .00001). CSM patients had a lower risk of receiving an oral opioid prescription (RR of 0.68 [95% CI: 0.68-0.69; P < .00001]).
Conclusions: This study found that adults with sciatica who initially received CSM had a lower risk of an ORADE compared to matched controls not initially receiving CSM, likely explained by a lower probability of opioid prescription. These findings corroborate existing practice guidelines which recommend adding CSM to the management of sciatica when appropriately indicated.
From the FULL TEXT Article:
There is more like this @
LOW BACK PAIN Section and the
ADVERSE EVENTS Section and the
OPIOID EPIDEMIC Section
Introduction
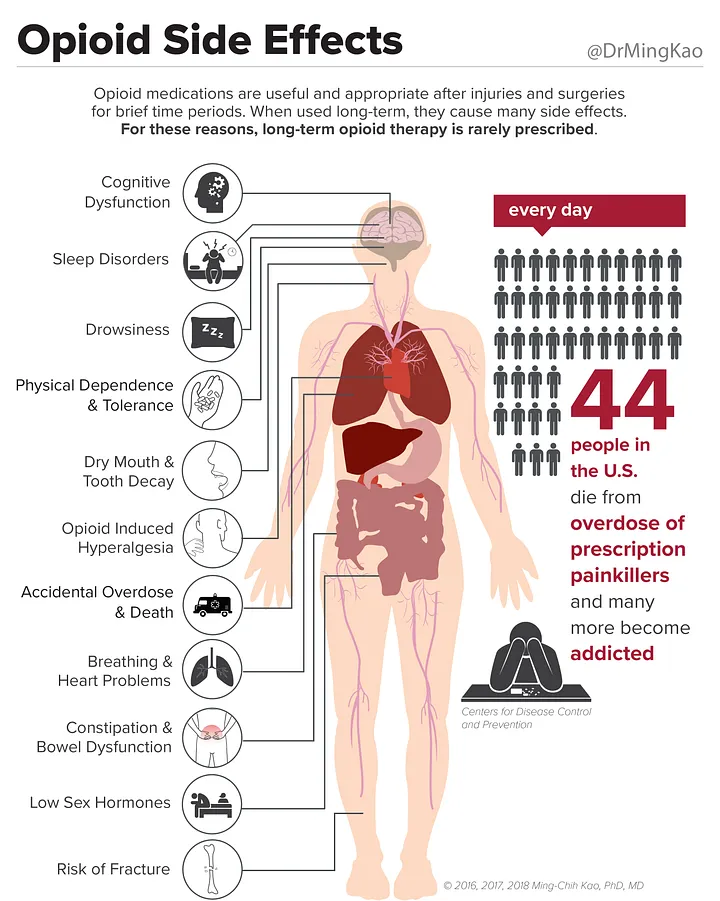
Opioids are narcotic analgesic medications that are often used to treat painful conditions such as sciatica, a radiating pain from the lumbar spine into the lower extremity, most often caused by irritation of lumbosacral nerve root(s). Despite limited evidence of efficacy in this condition, opioids are frequently prescribed to treat sciatica. [1–4] Opioids may cause a range of adverse effects commonly including constipation, dizziness, and sedation, and less often, nausea and vomiting. In addition, opioids have the potential for misuse, long-term use, dependency, addiction, and respiratory depression leading to death. [5] Opioid-related adverse drug events (ORADEs) are typically defined as moderate to severe adverse effects, such as opioid-related poisoning, overdose, and death. [5, 6]
The United States’ (US) Centers for Disease Control (CDC) and several recent clinical practice guidelines have discouraged prescribing opioids for acute musculoskeletal etiologies of low back pain [7, 8] while national health care systems have implemented opioid stewardship approaches involving interdisciplinary care and opioid safety initiatives. [9] As a result, the yearly percentage of US adults who received an opioid prescription has declined from 28% to 19% between 2008 and 2018. [10] Despite this, ORADEs remain relatively common. In one cohort study including 5684 subjects, emergency department encounters or hospitalizations for ORADEs affected 1.7% of patients newly prescribed a long-acting opioid, yielding an incidence rate of two to six per 100 person-years. [11] Concerningly, the yearly incidence of opioid overdose deaths in the US has gradually increased over the past two decades, most recently 25 per 100,000 people in 2021, although this estimate also includes deaths from non-prescription opioid use, particularly illicit fentanyl [12], which influences mortality statistics. As a result, this value does not represent deaths strictly from prescribed opioids.
Chiropractic spinal manipulation (CSM) is a form of manual therapy directed to the joints of the spine. Given its clinical effectiveness for treating sciatica [13], it is recommended by clinical practice guidelines for treatment of this condition. [14–18] Prior studies suggest that receiving CSM for spinal pain is associated with lower rates of opioid prescription compared to usual medical care [19, 20] and potentially reduces risk of any adverse drug event compared to conventional medical management in adults. [21, 22] For example, one study found the risk of any outpatient adverse drug event was 51% lower over 12 months in those receiving CSM versus those who did not. [21]
To date, no studies have specifically evaluated whether CSM is associated with a reduced likelihood of moderate to severe opioid-related adverse drug events (ORADEs) compared to usual medical care in any population. Our achieved aim was to examine this question using a real-world population of adults with sciatica. We hypothesized that adults receiving CSM for sciatica would have a lower risk of ORADEs over 12 months’ follow-up compared to propensity-matched controls not receiving CSM.
:Protocol for a Healthcare Systems Embedded Multisite Pragmatic Cluster-randomized Trialal")



Leave A Comment