

Radiologic Manifestations of Spinal Subluxations
We would all like to thank Dr. Richard C. Schafer, DC, PhD, FICC for his lifetime commitment to the profession. In the future we will continue to add materials from RC’s copyrighted books for your use.
This is Chapter 6 from RC’s best-selling book:
“Basic Chiropractic Procedural Manual”
These materials are provided as a service to our profession. There is no charge for individuals to copy and file these materials. However, they cannot be sold or used in any group or commercial venture without written permission from ACAPress.
Chapter 6: Radiologic Manifestations of Spinal Subluxations
This chapter describes the radiologic signs that may be expected when spinal subluxations are demonstrable by radiography. Through the years, there have been several concepts within the chiropractic profession about what actually constitutes a subluxation. Each has had its rationale (anatomical, neurologic, or kinematic), and each has had certain validity contributing to our understanding of this complex phenomenon.
You may review the full Chapter 6 @:
Kinetic Intersegmental Subluxations
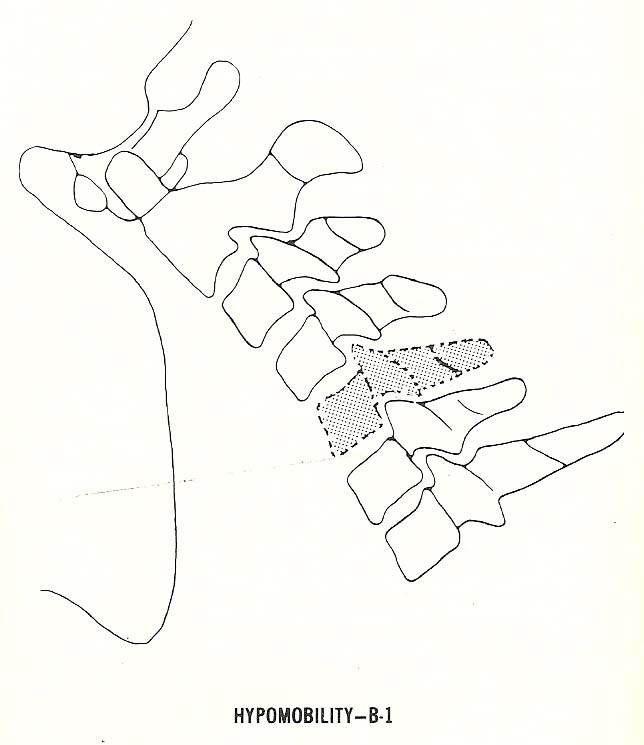
Segmental hypomobility, also called a “fixation subluxation” by many clinicians, may affect one or several motor units.
It is characterized by reduced motion of the “Spinal Motion Unit” (Please refer to Spinal Anatomy 101), which has been forced to the extreme of a range of motion (eg, flexion, extension, etc). See Figure 6.14. Stress views or videofluoroscopy are necessary to depict this and other kinetic subluxations radiographically, but motion palpation and some orthopedic tests may reveal their presence clinically.
Editor’s Note: In the following picture, the inferior facet of C5 fails to slide forwards and upwards upon the superior facet of C6. Because of that, the IVF cannot open more fully, and the spinous process of C5 fails to move away from the C6 spinous. All together, these are the classic signs of HYPO-mobility.
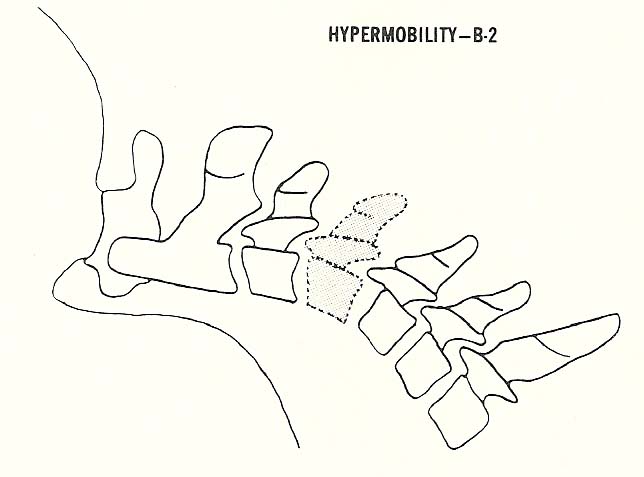
Hypermobility, called loosening of the vertebral motor unit by Earl Rich and Junghanns, may also be found at one or several levels. It is often found as a compensatory mechanism accompanying hypomobility (fixation) at one or more other levels in the kinematic chain.
Hypermobility (ie, an excessive range of motion) allows excessive range(s) of motion during flexion (Fig. 6.15). Again, this entity can be demonstrated by clinical means as well, but it takes stress radiography to document its presence objectively.
NOTE: If there is excessive translation on flexion/extension films (more than 3 mm), this is a classic sign of instability.
Read Steven Eggleston, DC, Esq’s article as it reviews the methodology for measuring spinal instability.
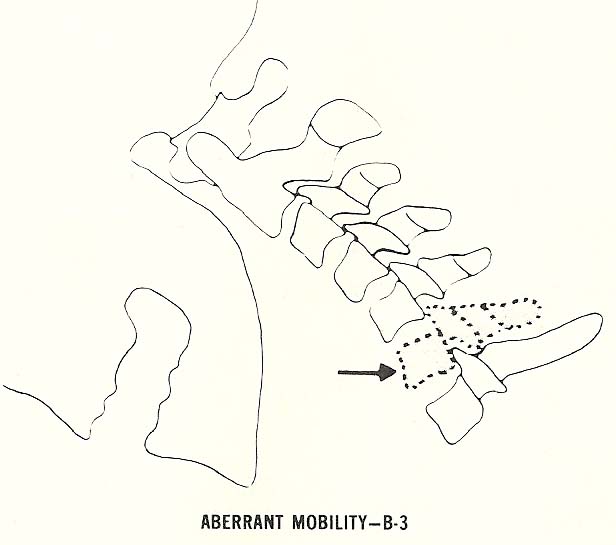
Aberrant motion exists when one or several vertebrae move in a way that is not in coordination with neighboring segments during some movement of the spine.
One vertebra, at least, is not in phase with the general movement of neighboring segments (Fig. 6.16). In this view, one segment is extending while the others are in flexion.
White & Panjabi, in their textbook “Clinical Biomechanics of the Spine” refer to this as “paradoxic motion”.
Static Intersegmental Subluxations
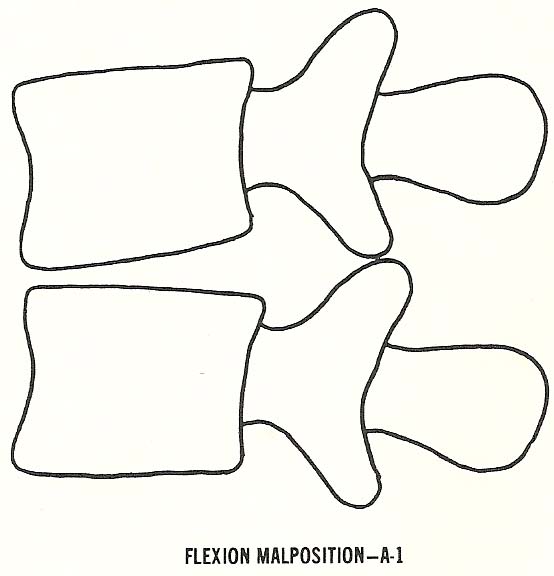
Flexion Malposition. In flexion subluxation, there is wedging of the disc space anteriorly as the vertebral bodies somewhat approximate one another anteriorly (Fig. 6.3).
Because of this, the spinous processes separate (open) and the inferior articular processes of the vertebra above glide upward upon the superior articular processes of the vertebra below. This elongates the intervertebral foramen (IVFs) so they appear larger in their vertical dimension.
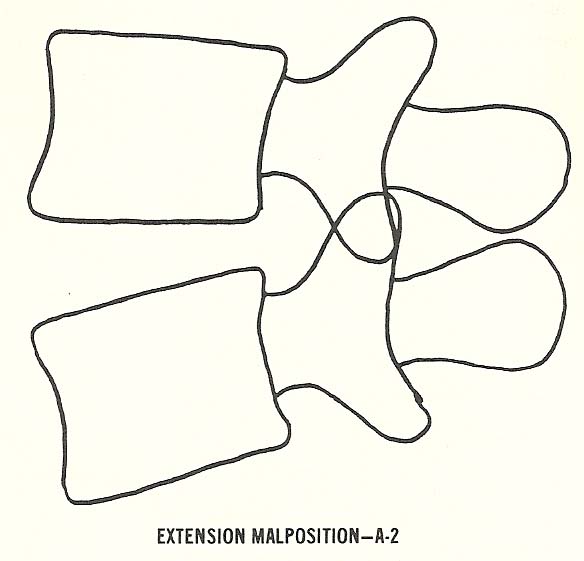
Extension Malposition. In this type of subluxation, which is one of the most commonly encountered (especially in the low back), the vertebral bodies approximate posteriorly and thus the disc narrows posteriorly (Fig. 6.4).
The posterior articulations show radiographic imbrication as the inferior articular processes of the vertebra above glide downward relative to the superior articular processes of the vertebra below. As the motion unit extends, the IVFs of the unit appear to become smaller in their vertical dimension.
You may review the full Chapter 6 @:


It is amazing that chiropractic care simplicity is still the foundation of our profession. It seems that so many chiropractors are looking for the better mouse trap when we have the gold standard at our fingertips!
I have always enjoyed the work of Dr. Schaefer. He writes very well and does an excellent job of making complex material understandable. My only concern with the above material is the detailed connection of specific motor unit dysfunctions and degenerative pathology with a poorly defined terms such as subluxation. There are innumerable causes of the above categories. Yet, we tend to simplify the issue by dropping everything into the subluxation rubric. For example, degenerative disc disease can be a result of trauma, chronic dysfunction, and aging to name a few. Is aging a subluxation? Why not simply call it what it is?
Hi Dr. Riggs
I don’t believe RCs posting suggests that the subluxation is the only cause of degenerative disease…it’s merely one cause. However, many of the causes you mention (such as trauma or chronic dysfunction) have as their initiating mechanism the joint fixation that is at the root of subluxation.
A fixation by itself has no clinical meaning, but a PERSISTENT fixation interferes with normal joint nutrition and clearance of waste products, causing an adverse impact on chondrocytes. As those cells die off and joint space reduces, the body mobilizes minerals to stabilize the joint (osteophytes). This combined process is what is referred to as the subluxation COMPLEX. If you have a term you prefer, that’s fine, but there’s no debating that fixation is the underlying cause of the process, and that adjusting/manipulation can halt those changes.
It’s equally important that chiropractors know and understand the material in this posting, particularly since some schools under-emphasize this material in their curricula.
Finally, I don’t believe subluxation is as poorly defined as you seem to believe. It’s a theory, but there is significant literature that supports it. Please refer to the following page for more on this topic:
What is The Chiropractic Subluxation?