
Spinal Manipulative Therapy-specific Changes in Pain Sensitivity in Individuals with Low Back Pain
SOURCE: Journal of Pain 2014 (Feb); 15 (2): 136–148
Joel E Bialosky, PT, PhD, Steven Z George, PT, PhD, Maggie E Horn, Donald D Price, PhD, Roland Staud, MD, and Michael E Robinson, PhD
Department of Physical Therapy,
Center for Pain Research
and Behavioral Health,
University of Florida,
Gainesville, Florida.
Spinal manipulative therapy (SMT) is effective for some individuals experiencing low back pain; however, the mechanisms are not established regarding the role of placebo. SMT is associated with changes in pain sensitivity, suggesting related altered central nervous system response or processing of afferent nociceptive input. Placebo is also associated with changes in pain sensitivity, and the efficacy of SMT for changes in pain sensitivity beyond placebo has not been adequately considered. We randomly assigned 110 participants with low back pain to receive SMT, placebo SMT, placebo SMT with the instructional set “The manual therapy technique you will receive has been shown to significantly reduce low back pain in some people,” or no intervention.
Participants receiving the SMT and placebo SMT received their assigned intervention 6 times over 2 weeks. Pain sensitivity was assessed prior to and immediately following the assigned intervention during the first session. Clinical outcomes were assessed at baseline and following 2 weeks of participation in the study. Immediate attenuation of suprathreshold heat response was greatest following SMT (P = .05, partial η2 = .07). Group-dependent differences were not observed for changes in pain intensity and disability at 2 weeks. Participant satisfaction was greatest following the enhanced placebo SMT.
This study was registered at www.clinicaltrials.gov under the identifier NCT01168999.
PERSPECTIVE: The results of this study indicate attenuation of pain sensitivity is greater in response to SMT than the expectation of receiving an SMT. These findings suggest a potential mechanism of SMT related to lessening of central sensitization and may indicate a preclinical effect beyond the expectations of receiving SMT.
There are more articles like this @ our:
Low Back Pain and Chiropractic Page and the:
KEYWORDS: Central sensitization; low back pain; manual therapy; placebo; spinal manipulation
From the FULL TEXT Article:
Introduction
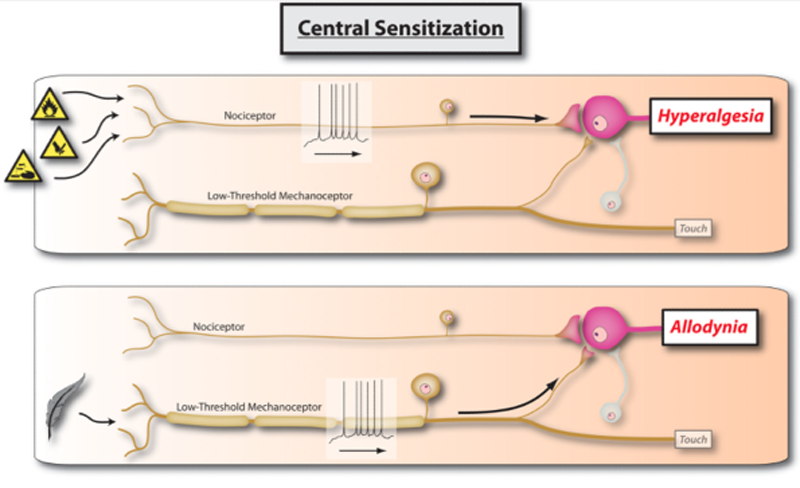
Low back pain (LBP) is a significant public health problem with lifetime incidence rates up to 90% [89] and loss of work production estimated at 7.4 billion dollars for workers in the United States between the ages of 40 and 65. [70] Chronic LBP, similar to other chronic pain conditions (e.g. fibromyalgia), is associated with altered pain processing [42, 63] suggesting a mechanism related to central sensitization of pain. [56, 76] Specifically, chronic LBP is associated with generalized pain sensitivity [42] and cortical responses to painful stimuli differing from those observed in healthy individuals. [2, 28] Central sensitization is considered a factor in the progression of acute pain to chronic pain and the maintenance of chronic pain. [71] Subsequently, attenuation of central sensitization may represent a treatment target. [81]
Spinal manipulative therapy (SMT) is an effective [13–15, 31] complementary and alternative medicine intervention for some individuals experiencing LBP. SMT is recommended by many LBP clinical practice guidelines; [21] however, not all clinical practice guidelines support SMT and variability exists between those which do suggesting a need for stronger evidence. [57] Improved understanding of the mechanisms of SMT could enhance clinical effectiveness and clarify the variability in the present literature. LBP is a heterogonous condition for which the anatomical basis is commonly unidentifiable. [26] Subsequently, a pathoanatomical diagnosis is generally not helpful for guiding treatment [24] and identifying subgroups of individuals with LBP most likely to benefit from a specific intervention is a research priority. [27] Clarifying the mechanisms of SMT could assist in identifying key features of individuals with LBP likely to respond to these interventions allowing more efficacious clinical application.
SMT is associated with changes in pain sensitivity [19, 61] suggesting a mechanism related to attenuation of central sensitization. [10] SMT results in increased mechanical pain thresholds in individuals with neck pain [23, 88] and lateral epicondylalgia [30] and attenuation of suprathreshold heat response. [8, 9, 38] Consequently, the clinical effectiveness of SMT could result from lessening of central sensitization.
Placebo is associated with robust analgesia [85] enhanced by expectation for pain relief. [66] For instance, saline is associated with analgesia in patients with fibromyalgia [69] and irritable bowel syndrome [86] believing they received a pain relieving drug. Clinical outcomes related to interventions for pain result from both intervention specific and placebo mechanisms. [91] This point is exemplified in open- hidden paradigm studies in which a known analgesic agent is provided in an open manner or through hidden infusion resulting in greater analgesia when openly administered. [5, 16] Expectation is also influential in outcomes related to complementary and alternative medicine interventions. For example, a study comparing the efficacy of massage and acupuncture for individuals with LBP observed a moderating effect of expectation. [54]
Read the rest of this Full Text article now!



Leave A Comment